AS01 adjuvant in M72 vaccine: from malaria research to tackling tuberculosis
By Impact Global Health 18 June 2026
Context
Every breakthrough in global health sends ripples that reach far beyond borders. In an era of fiscal tightening and inward-facing policy priorities, investments in global health R&D are under increasing pressure. Yet these investments are among the most powerful drivers of innovation, economic growth, and resilience – not just for low- and middle-income countries (LMICs), but for high-income countries (HICs) as well. In the Ripple Effect project 1.0, Impact Global Health demonstrated that $71 billion in global health R&D funding from 2007– 2023 catalysed $511 billion in GDP growth, 643,000 jobs, and 20,000 patents in HICs, a multiplier effect proving that global health investment drives domestic prosperity as well as global health outcomes. Building on this, the Ripple Effect 2.0 examined this dynamic through case studies of innovations initially developed for LMIC needs that later delivered measurable health and economic benefits in HICs. Now, the Ripple Effect 3.0 project extends this work by applying the same approach to five additional products, further strengthening the evidence base.
This case study focuses on the benefits of the AS01 adjuvant, initially advanced through GSK and PATH’s RTS,S malaria vaccine global health research programme, before being adopted across a range of diseases and vaccines candidates, including to enhance the effectiveness of the M72/AS01E candidate vaccine for tuberculosis (TB). This has big potential in HICs where ageing and diverse populations who were exposed to higher rates of TB previously are more at risk for developing active TB.
- An LMIC-focused malaria innovation has the potential to protect against TB in adults worldwide. AS01, an adjuvant originally developed for malaria vaccines, is now powering M72/AS01E, one of the most advanced candidates that could become the first new TB vaccine in more than a century.
- By 2050, the M72/AS01E vaccine is projected to prevent over 420,000 cases of TB, save 52,000 lives, and avert nearly 764,000 DALYs in the UK, US, Europe and Japan.
- The societal and economic returns are significant, with $176 billion in value from healthy years gained and $5.6 billion in health-system cost savings across all four markets.
- For every dollar spent on the M72/AS01E vaccination programme, health systems save an estimated $28 in avoided treatment costs.
What is tuberculosis and why do we need a new vaccine?
Despite being preventable and curable, tuberculosis (TB) causes more than a million deaths every year and remains one of the world's most persistent infectious disease challenges. Around a quarter of the global population carries latent TB infection (LTBI) - a dormant form of the bacteria that causes no symptoms and cannot be spread to others. When someone breathes in Mycobacterium tuberculosis, the bacterium that causes TB, the immune system typically holds the infection in check rather than clearing it entirely. For most people, it stays that way for life. But ageing, HIV status, diabetes or certain medications can tip the balance, allowing dormant infection to reactivate into infectious TB disease. In high-income countries like the UK, US, Europe and Japan, TB today is driven less by ongoing spread but more by a large ‘silent reservoir’ of past infection. Many cases occur in older adults and in migrants born in countries with high rates of TB infected years – sometimes decades – earlier, with the bacteria becoming active later in life as the immune system weakens.
The only registered TB vaccine, BCG, is over a century old. It protects young children but offers little protection against pulmonary TB in adults, the form that causes the most deaths. A promising new vaccine, M72/AS01E – which utilises the AS01 adjuvant – has demonstrated efficacy in adults with latent TB infection and is now advancing through trials to establish its broader protective potential to all adults. It represents a real opportunity to reduce TB in the populations that current strategies have failed to reach, including those with greatest burden in high-income country settings.
Innovation pathway
The story of M72/AS01E begins not with tuberculosis, but with malaria. The AS01 adjuvant was initially developed as part of global health research to develop malaria vaccines and was ultimately included in the first approved malaria vaccine, Mosquirix (RTS,S/AS01) in 2021. Designed to enhance both humoral and cellular immune responses across age groups, AS01 was recognised as an adaptable platform with applications beyond malaria. Its performance with other vaccine candidates, including in our case studies showcasing its potential in Shingrix (for shingles) and Arexvy (for respiratory syncytial virus infection), demonstrates its ability to strengthen immune responses to a range of pathogens.
Recognising AS01's versatility, GSK partnered with Aeras and the International AIDS Vaccine Initiative (IAVI) to pair AS01 with M72, a protein derived from two tuberculosis antigens present during both active disease and latent infection. In 2019, a landmark trial across Kenya, South Africa and Zambia demonstrated that M72/AS01E reduced the risk of active pulmonary TB by around 50% in adults with LTBI; the first significant proof of TB vaccine efficacy in over a century. GSK subsequently licensed the candidate to the Gates Medical Research Institute, which launched a pivotal Phase 3 trial in March 2024. Notably, the Phase 3 trial is enrolling adults regardless of LTBI status, with the potential to establish M72/AS01E as a broadly applicable adult TB vaccine with worldwide application.
The trajectory of AS01, from malaria research to the most advanced new TB vaccine in a century, illustrates how investment in global health R&D can generate tools with far-reaching benefits, including in high-income countries well beyond the original malaria use case.
Health impact in the EU, UK, US and Japan
Across the EU, UK, US and Japan – key HIC markets selected in this study for their substantial impact and strong data availability – we estimate that M72/AS01E could prevent 423,000 TB cases, save over 52,000 lives, and avert almost 764,000 DALYs by 2050.
Japan accounts for the largest share of projected lives saved; over 31,000 of the 52,000 total across the four markets. Three factors explain this. Japan has historically had a higher TB incidence than other high-income countries, meaning a larger share of its older population carries latent infection acquired decades ago. Second, Japan has a significantly higher case fatality rate than the other markets, as sourced from the GBD- around 18%, compared to 10% in the US, 9% in Europe, and 4% in the UK. In practical terms, this means that when TB does develop in Japan, patients are far more likely to die from it. As a result, the vaccine is projected to prevent a similar number of TB cases in Europe and Japan but saves roughly twice as many lives in Japan. Finally, with a rapidly ageing population, Japan represents precisely the setting where an effective adult TB vaccine would have the greatest impact.
Table 1: Potential health impact from M72/AS01E in the EU, UK, US, and Japan
Figure 1: Estimated TB cases averted by M72/AS01E vaccine
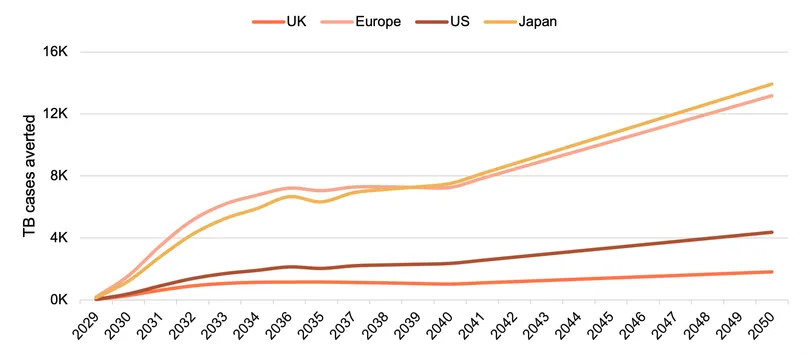
In the UK and US, where TB incidence is lower, the burden is increasingly concentrated among older adults and people born outside of those countries, who face higher reactivation risk and limited vaccine protection. By 2050, vaccination could avert more than 25,000 cases in the UK and 54,000 in the US, delivering meaningful benefits in two of the world’s most resource-intensive health systems, where even modest reductions in TB cases would generate substantial savings in treatment costs and hospital resources.
Across all four settings, the thread is the same: a shared ageing population carrying decades-old latent infection, with no vaccine protection and a growing window of reactivation risk is poised to benefit from M72/AS01E as a uniquely positioned candidate to close this gap. If M72/AS01E is also proven to protect those without LTBI in the current Phase 3 trial, the health gains could be even more significant.
Economic Impact in the EU, UK, US and Japan
Being alive and in good health has a value to the individual and to society. Using the Value of a Statistical Life approach, we estimated the societal gains from 764 thousand DALYs averted – discounted to reflect the slightly lower value associated with future years lived – to be worth $176 billion[1] across our four markets.
Table 2: Potential health system cost savings (USD 2025) from M72/AS01E
Figure 2: Total health system savings over time from M72/AS01E
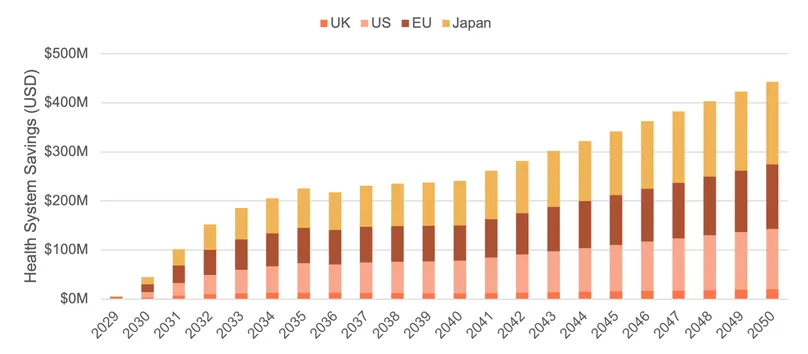
Rolling out the M72/AS01E vaccine is estimated to save health systems significantly more money than it costs to deliver – meaning that in addition to its health benefits, it is financially attractive for the health system.
The savings arise from avoiding the cost of treating tuberculosis. TB treatment is expensive: even the standard drug-susceptible (non-resistant) form costs between $7,000 and $25,000 per patient, depending on the country, while drug-resistant forms, which affect a small minority of patients, can cost hundreds of thousands of dollars per case. Across the 423,000 cases averted over the modelling period, the avoided treatment costs total an estimated $5.6 billion – $1.7 billion for Europe, $2.0 billion for Japan, $1.5 billion for the United States, and $277 million for the United Kingdom. Japan's figure is disproportionately large relative to its population size, reflecting the high prevalence of latent TB infection among its large elderly adult population.
The cost of delivering the vaccine, by contrast, is estimated at just over $200 million. This is relatively low because the current programme targets only adults known to carry latent TB infection, rather than vaccinating the general population, meaning the total number of doses required is relatively low. This is aligned with the current evidence base from the 2019 trial. If the Phase 3 trial shows promise of protection for the general population the cost of delivering this rollout will be higher.
Because no price has yet been set for M72/AS01E, procurement costs are estimated using Shingrix as a benchmark. Shingrix is made by the same manufacturer and uses the same adjuvant technology. We applied a 40% downward adjustment to reflect the assumption that procurement of a TB vaccine is expected as a public health tool rather than a commercial product. Even without this reduction though, the programme would still be cost saving.
The result is that for every dollar spent on the vaccination programme, health systems save an estimated $28 in avoided treatment costs – with the cost of delivery remaining sensitive to the assumed vaccine price, given that no market price for M72/AS01E has yet been established.
[1] For ease of comparison, all monetary values are reported in inflation-adjusted 2025 US dollars
Conclusions
The story of AS01 and M72 illustrates how global health research works as a cycle of shared innovation and shared returns. An adjuvant technology developed to tackle malaria in low-income settings now underpins what could become the first new TB vaccine in over a century – with broad applicability and impact in HIC settings too – demonstrating that investments made to address neglected diseases rarely stay contained to the populations they were first designed to help.
If M72/AS01E succeeds in Phase 3 and gains approval, it could save lives, ease pressure on health systems, and show how investment in neglected disease R&D can deliver benefits far beyond the populations and diseases it was originally intended to address.
Key assumptions
The projected health impact of M72/AS01E vaccination follows clear epidemiological and demographic logic. This analysis builds on modelling originally conducted for our Impact of Global Health R&D report and Global Plan to End TB, developed in collaboration with Avenir Health and extended to 2050 for this analysis.
Our starting point is the deaths averted and DALYs estimated in the Evidence for Impact project. Those estimates assumed a vaccine efficacy of 60%; we adjusted this down to 49.7% to reflect the three-year results reported in the Phase 2 trial. While efficacy was slightly higher at the 2.3-year interim analysis (54.0%), the difference is not statistically significant, and confidence intervals overlap substantially. From the adjusted deaths averted figures, we retrospectively estimated TB cases averted using age and country-specific case fatality rates drawn from the Global Burden of Disease, applied to those aged 15–85 rather than the general population, reflecting that TB in these four markets is concentrated among older age groups and to reflect the target population of the vaccine. The CFRs used are: UK 4.4%, USA 9.6%, Europe 8.7% and Japan 18.2%. Doses administered are calculated by dividing cases averted by vaccine efficacy, assuming coverage trajectories built into the original modelling. Protection is assumed to last 10 years, consistent with our previous modelling and aligning with vaccine aims in the Global Plan. Vaccine rollout is modelled from 2029, updated from the Global Plan's original 2027 assumption to reflect the Phase 3 trial launch in March 2024 and the likely regulatory pathway.
To estimate health system cost savings, we collected treatment costs for each region and grouped them by drug resistance type: drug-susceptible, MDR, and XDR-TB. This reflects the substantial cost differences between these categories. Although drug-resistant TB represents only a small share of cases in all four regions, it is far more expensive to treat than drug-susceptible TB, so including it materially affects the weighted average cost per case. Germany was used as a proxy for Europe, because it has the strongest peer-reviewed cost data among EU member states. All costs were converted to USD and inflated to a 2025 base year using the US Bureau of Labour Statistics Medical Care Consumer Price Index. We then used current national drug resistance surveillance data for each region to calculate a weighted average cost per averted case.
The cost of delivering the vaccine was estimated using Shingrix – a vaccine developed by the same manufacturer using the same AS01E adjuvant platform and two-dose schedule – as a pricing analogue, adjusted downward by 40% to reflect the assumption that procurement of a TB vaccine is expected as a targeted public health tool rather than a commercial product. Country-specific administration fees were added based on published sources for each setting. A linear price depreciation is applied from 2039 onwards, reflecting anticipated post-patent price reductions, with the vaccine reaching 65% of its base-case price by 2050.
The model captures all vaccination costs across the 2029–2050 period, but not the full downstream health benefits: individuals vaccinated in the final years of the modelling window will continue to be protected beyond 2050, avoiding cases and their associated treatment costs that fall outside the model's horizon. Accounting for these additional post-2050 benefits would further strengthen the cost-effectiveness and health impact estimates, which are already evident across all four regions.
For full data, visuals and methodology, visit: https://www.impactglobalhealth.org/insights/report-library/ripple-effect-3