AS01 adjuvant in Arexvy: from malaria research to protecting ageing populations
By Impact Global Health 18 June 2026
Context
Every breakthrough in global health sends ripples that reach far beyond borders. In an era of fiscal tightening and inward-facing policy priorities, investments in global health R&D are under increasing pressure. Yet these investments are among the most powerful drivers of innovation, economic growth, and resilience – not just for low- and middle-income countries (LMICs), but for high-income countries (HICs) as well. In the Ripple Effect project 1.0, Impact Global Health demonstrated that $71 billion in global health R&D funding from 2007– 2023 catalysed $511 billion in GDP growth, 643,000 jobs, and 20,000 patents in HICs, a multiplier effect proving that global health investment drives domestic prosperity as well as global health outcomes. Building on this, the Ripple Effect 2.0 examined this dynamic through case studies of innovations initially developed for LMIC needs that later delivered measurable health and economic benefits in HICs. Now, the Ripple Effect 3.0 project extends this work by applying the same approach to five additional products, further strengthening the evidence base.
This case study focuses on the benefits of the AS01 adjuvant, initially advanced through the RTS,S malaria vaccine research programme, before being adopted to enhance the effectiveness of GSK’s ‘Arexvy’ respiratory syncytial virus (RSV) vaccine in older people.
- A malaria-driven innovation is now protecting ageing populations in high-income countries: AS01, an adjuvant originally developed for malaria vaccines, is powering Arexvy, the respiratory syncytial virus vaccine with the potential to deliver major health and economic gains across high-income countries, including the US, Europe, Japan and the UK.
- By 2050, Arexvy is projected to prevent around 15 million cases of RSV acute respiratory infection, save nearly 107,500 lives, and avert 1.3 million disability adjusted-life years (DALYs) in HICs.
- The societal and economic returns are significant with nearly $310 billion in value from healthy years gained and $20 billion in health-system cost savings across all four markets by 2050.
What is respiratory syncytial virus and why do we need a new vaccine?
Respiratory syncytial virus (RSV) is a common respiratory pathogen that causes seasonal outbreaks, ranging from mild upper respiratory tract illness to severe lower respiratory tract disease. While RSV infection is often mild in healthy young adults, it can cause serious disease at both ends of the age spectrum. It is a major cause of severe respiratory illness in infants and young children, particularly those under five, and it also poses a substantial threat to older adults and people with underlying conditions such as COPD or heart failure.
Arexvy was initially developed and approved to prevent RSV lower respiratory tract disease in adults aged 60 and over, addressing a major unmet need in this population. Its indication has since expanded to include adults aged 18 to 59 who are at increased risk of severe RSV disease. However, the health and economic analysis presented here models impact in older adults, reflecting the original approval population, the larger adult burden, and the primary vaccination market for Arexvy. In the US alone, RSV leads to an estimated 160,000 hospitalisations and up to 10,000 deaths annually among older adults.
Until 2023, there was no approved vaccine to protect this older adult population following decades of unsuccessful attempts. Arexvy addressed this gap by combining a stabilised prefusion F protein antigen with GSK’s malaria-based AS01E adjuvant system, achieving over 80% efficacy against symptomatic RSV disease in its first season and becoming the world’s first approved RSV vaccine for older adults.
Innovation pathway
The AS01 adjuvant was created as part of global health research aimed at developing vaccines for malaria and was ultimately included in the first approved malaria vaccine, Mosquirix (RTS,S/AS01), developed by GlaxoSmithKline in collaboration with PATH. Designed to enhance both humoral and cellular immune responses across age groups, AS01 was recognised as an adaptable platform technology with potential applications beyond malaria. Its performance with other vaccine candidates demonstrated its ability to strengthen immune responses to a range of different pathogens.
Building on this foundation, GSK incorporated AS01 into several vaccines: Shingrix, as we have illustrated in a prior case study, but also Arexvy for respiratory syncytial virus (RSV) and M72 for tuberculosis. By pairing AS01E – a variant of the AS01 adjuvant system – with the RSV prefusion F antigen (RSVPreF3), Arexvy was able to elicit a strong and durable immune response against RSV lower respiratory tract disease in older adults. Approved in 2023, it is currently recommended for adults aged 60 and over and is administered as a single intramuscular dose. Since its introduction, Arexvy has been approved in over 70 countries and has become the first RSV vaccine available for older adults, addressing a significant unmet need in a population vulnerable to severe RSV-related hospitalisations and death.
The trajectory of AS01, from global health research to a platform now used in vaccines worldwide, demonstrates the potential multi-directional value of investments in global health R&D. The role of the adjuvant in Arexvy, the focus of this case study, and in other products such as Shingrix for shingles and the advancing M72 tuberculosis vaccine candidate, highlights how a single innovation can ultimately help address multiple public health priorities, including in HICs far beyond the original LMIC-focused use case.
Health impact in the EU, UK, US and Japan
Across the EU, UK, US and Japan – key HIC markets selected in this study for their substantial impact and strong data availability – we estimate that by 2050 Arexvy will prevent 15.4 million RSV acute respiratory infection (ARI) cases, save about 107,500 lives, and avert 1.3 million DALYs. The health impact is largely driven by population size and age structure – the larger and older the population, the more harm done by RSV ARI and the larger the health benefits of a vaccine like Arexvy. Another key variable is the coverage of Arexvy compared to its competitors in each respective market. In each region, the model asks a different question: in the US and EU, how much additional value does Arexvy deliver in a market shared with Abrysvo and mResvia – other RSV vaccines; in the UK, what would be the incremental benefit if the NHS were to switch from Abrysvo to Arexvy; and in Japan, how Arexvy performs against mResvia as the only alternative.
Table 1: Potential health impact from Arexvy in the EU, UK, US, and Japan
While RTS,S is estimated to avert 194 million DALYs and save 2.2 million lives from malaria by 2040, Arexvy addresses a distinct gap: until 2023, no vaccine existed against RSV in older adults despite it being the leading cause of viral pneumonia hospitalisations in this age group. The same adjuvant platform that transformed child survival from malaria through RTS,S is now reducing severe respiratory disease burden in ageing, high-income populations.
Figure 1: Estimated RSV acute respiratory infection (ARI) cases averted by Arexvy
%20cases%20averted%20by%20Arexvy-808x611.webp)
Economic Impact in the EU, UK, US and Japan
Being alive and in good health has a value to the individual and to society. Using the Value of a Statistical Life approach, we estimated the societal gains from 930,000 DALYs averted to be worth close to $310[1] billion across our four markets.
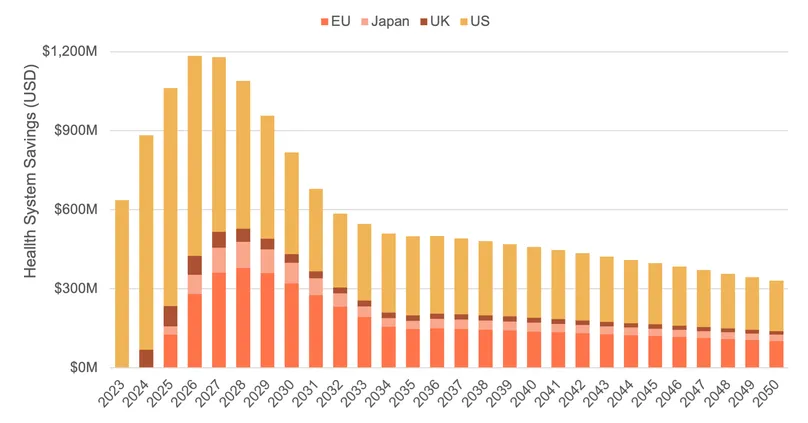
Rolling out Arexvy also generates substantial savings for health systems, primarily through fewer hospitalisations and GP visits. The estimated 15.4 million RSV-initiated ARI cases averted, including 1.4 million hospitalisations prevented, are projected to save around $16 billion in health system costs, with approximately three quarters of these savings driven by avoided hospitalisations. The largest savings are estimated in the US (around $10 billion), reflecting the higher cost of healthcare services and treatment compared to other countries.
Delivering the new vaccine also, however, comes at a cost. Based on projected vaccine prices and administration costs, we estimate the net incremental cost of Arexvy vaccine delivery at $25.6 billion across the four markets included in our analysis, compared to alternative RSV vaccination scenarios. To be more precise, the net cost of rolling out Arexvy is estimated at $12 billion in the US, $9.8 billion in Europe, nearly $2 billion in the UK, and $1.8 billion in Japan.
In all markets, the cost of rolling out the vaccine exceeds the direct health-system savings. This is typical for vaccines, which require substantial upfront investment to generate long-term health benefits. In the US, the gap is narrow: vaccination costs of $12.0 billion are largely offset by $9.6 billion in health-system savings, meaning the programme recoups roughly 80 cents of every dollar spent through avoided healthcare costs alone – before accounting for the broader health gains. In Japan, $1.1 billion in savings offsets around two-thirds of the $1.8 billion vaccination outlay. In Europe and the UK, the savings-to-cost ratio is lower, though still substantial: Europe sees $4.7 billion in savings against $9.8 billion in costs, while the UK sees $0.8 billion against $2.0 billion.
But these estimates are also conservative: they do not account for cases averted after 2050 by vaccinations delivered before that date, which would continue to generate health-system savings beyond our modelling horizon.
Arexvy is projected to deliver significant health benefits across all four markets at a manageable programme cost, with the US coming closest to a cost-neutral position. However, the cost of delivering the vaccine remains highly sensitive to assumptions around vaccine coverage and changes in price per dose over time. Steeper post-patent price reductions than those incorporated in our model would further reduce the net cost of vaccination across all markets.
Table 2: Potential health system cost savings (USD 2025) from Arexvy
Figure 2: Total health system savings over time from Arexvy
[1] For ease of comparison, all monetary values are reported in inflation-adjusted 2025 US dollars
Conclusions
Arexvy illustrates how sustained investment in proven LMIC-disease focused interventions can unlock compounding returns across different disease areas and populations. The AS01 adjuvant system – originally developed for malaria, deployed at scale through Shingrix against shingles, and now powering Arexvy for RSV and the development of M72 tuberculosis vaccine candidate in Phase III trials – continues to find new applications decades after its inception. By helping to close a long-standing gap in protection for older adults against severe RSV disease, Arexvy reduces avoidable illness, hospitalisations, and deaths, while also demonstrating how global health R&D can create value beyond its original disease focus. The broader lesson is clear: investments made to solve urgent global health challenges can continue to generate health and economic benefits long after their first application.