From targeted solution to global maternal health asset: the JADA System
By Impact Global Health 19 January 2026
Context
Every breakthrough in global health sends ripples that reach far beyond borders. In an era of fiscal tightening and inward-facing policy priorities, investments in global health R&D are under increasing pressure. Yet these investments are among the most powerful drivers of innovation, economic growth, and resilience, not just for low- and middle-income countries (LMICs), but for high-income countries (HICs) as well. Impact Global Health has demonstrated that $71 billion in global health R&D funding from 2007– 2023 catalysed $511 billion in GDP growth, 643,000 jobs, and 20,000 patents, a multiplier effect proving that global health investment drives domestic prosperity. The Ripple Effect 2.0 project further examines this dynamic through three case studies of innovations originally developed for LMIC needs that later delivered measurable health and economic benefits in HICs. Building on this wider evidence of cross market benefits, this case study turns to postpartum haemorrhage (PPH).
Each year, millions of women experience PPH, resulting in about 70,000 maternal deaths globally1 and accounting for 12% of all maternal deaths in the USA2. Beyond its health impact, PPH imposes a significant economic burden on patients and the health system, with an estimated cost of $1.8 billion in the US in 20193. This case study focuses on the benefits of the JADA System – a device designed to stop bleeding by inducing a gentle vacuum in the uterus uterine device – for the rapid control of PPH in the USA.
1 Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Heal. 2014;2(6):323– 33. https://doi.org/10.1016/s2214-109x(14)70227-x
2 World Health Organisation. WHO postpartum haemorrhage (PPH) summit. 2022
3 O'Neil SS, Platt I, Vohra D, Pendl-Robinson E, Dehus E, Zephyrin L, et al. Societal cost of nine selected maternal morbidities in the United States. PLoS One. 2022;17(10):e0275656
Innovation pathway
Stopping PPH quickly is critical to prevent escalation, including surgery, blood transfusions, and death. The Bakri balloon and other improvised devices have been around for many years – used as lifesaving options in places where access to surgery and drugs like oxytocin is limited or non-existent. This has saved countless women’s lives, nearly all of them in LMICs.
The success of PPH devices, particularly balloon tamponades like the Bakri balloon, has helped pave the way for the evolution of newer PPH devices, including the JADA System. The JADA, instead of applying positive pressure to control uterine bleeding, it applies gentle negative pressure through a suction device. It is minimally invasive, easy to deploy, and acts within three minutes, offering critical advantages in emergency obstetric care where time, skills, and surgical capacity may be limited.
JADA demonstrated high effectiveness (94%)4 in controlling bleeding without the need for further intervention and was approved by the US FDA in 2020. Although it is currently recommended and used as a second line treatment when standard PPH care (with uterotonics and uterine massage) is insufficient, its FDA approval represents a significant advancement in maternal care. By rapidly controlling bleeding and reducing the need for more invasive procedures, JADA has the potential to help address the unacceptably high rates of maternal mortality in the US, particularly amongst women with limited access to healthcare. This innovation could be gamechanger in improving outcomes and equity in maternal health.
- Building on decades of PPH device innovation driven by LMIC needs, the JADA System now has the potential to deliver significant health and economic benefits in the US.
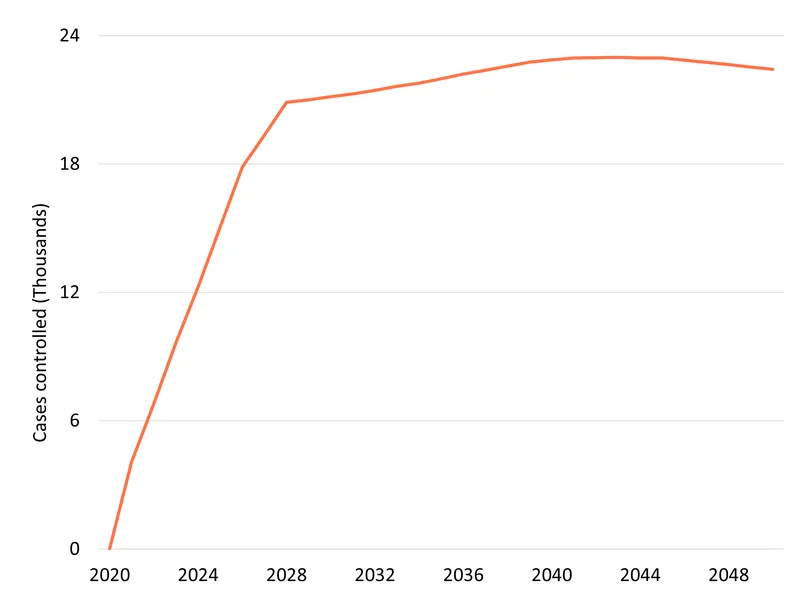
- By 2050, The JADA System is projected to control close to 597,000 additional cases of severe maternal bleeding, saving 1,000 lives, and averting 21 thousands DALYs in the USA.
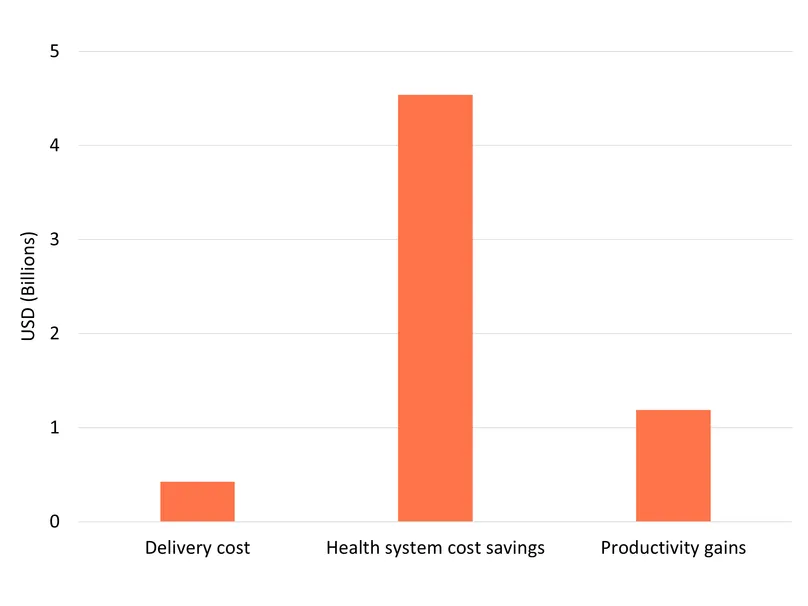
- The societal and economic returns are also significant: nearly $11 billion in value from healthy life years gained, $4.5 billion in health-system cost savings and $1.2 billion in productivity gains in the USA alone.
4 https://organonpro.com/en-us/product/the-jada-system/clinical-evidence/
Health impact in the USA
The projected number of PPH cases in the USA (extrapolating from the trend in case numbers through to 2023) is estimated at 4.5 million between 2020 and 2050. The great majority of these cases will be managed using just the standard of care but a subset will require a device – either JADA, or, in its absence, a balloon tamponade – to control the haemorrhage. So, while JADA would only ever be administered to this high need subgroup, we estimate that by 2050, after a period over which it gradually replaces balloons, JADA will be used to successfully control bleeding in 596,963 PPH cases. JADA’s much greater reliability in averting high volumes of blood loss means that, where it is used, it will radically reduce the maternal deaths still occurring each year from PPH particularly in more vulnerable population groups in the USA. Based on our modelling, JADA is expected to avert 919 deaths (out of the 1,341 which would occur without it), resulting in 20,514 discounted DALYs averted.
Economic impact
Being alive and in good health has a value to the individual and to society. Using the Value of a Statistical Life (VSL) approach, which approximates that value mostly based on how much people need to be paid to take on risky jobs, we estimate the societal gains from the 20,514 projected DALYs averted to be worth close to $11 billion5. In addition to the value of the life years saved, the future labour performed by mothers who would have died without JADA add up to an estimated at $1.2 billion by 2050.
Scaling up JADA and slowly replacing the Bakri Balloon also generates substantial cost savings for health systems, mainly due to reduction in direct treatment costs, blood transfusion costs, hospital stays, and intensive care costs. A study conducted in the US showed that the JADA System compared to the Bakri Balloon for high needs PPH cases saves about $7,000 per eligible patient. As a result, we estimate that the JADA System could save up to $4.5 billion to the health system.
These health system savings from averting negative outcomes need to be set against the additional cost of using JADA rather than the balloon. We estimate this additional extra cost at $425 million in the US, based on the roughly $500 per-patient price difference of the two treatments. Since this is far less than the savings to the health system, in the JADA System saves the health system money as well as delivering better health outcomes, giving it a negative incremental cost-effectiveness ratio (ICER) of around $259,000 saved per DALY averted. This ICER represents a high level of value. It highlights that JADA offers both improved health outcomes and lower overall spending. It also shows that the upfront cost is largely outweighed by the savings from avoided complications.
5 For ease of comparison, all monetary values are reported in inflation-adjusted 2025 US dollars
Conclusions
The use of the JADA System in the US illustrates how innovations initially conceived of to address global health challenges can generate far-reaching benefits beyond their original intent. The JADA System was developed by Alydia Health to provide a low-cost, rapid, and simple intervention for PPH, particularly in settings where access to surgery and drugs like oxytocin is limited or absent. It has since demonstrated improved performance compared to existing treatments, even in high-resource environments such as the US. This is another illustration that HICs, particularly those with high levels of health inequality, continue to experience the problems global health is designed to address.
By 2050, JADA is projected to control over half a million PPH cases, save close to a thousand lives, and avert more than 20,000 DALYs in the US alone. These health gains translate into nearly $11 billion in societal value and $4.5 billion in health-system savings – far exceeding the cost of introducing and scaling up the device. JADA’s impact reinforces a central message of the ripple effect: investments in global health R&D fuel breakthroughs that reduce costs and save lives across all regions.
Key assumptions
We used PPH case estimates from the GBD and applied a linear trend based on historical data to project PPH cases through 2050. We assumed that all PPH cases receive standard care (oxytocin and fluids) and that a subset of women (12%)6 require a device. Our analysis therefore compares the impact of JADA versus the Bakri balloon, with JADA gradually replacing the balloon over time to reach 90% coverage by 2050. In addition, we assume that JADA’s improved health outcomes, lower overall resource utilisation and reduced patient dwell times mean that it would be adopted more broadly for a proportion of women who would not otherwise have received any device. We assume this extra incremental uptake reaches an additional 6% of PPH cases by 2050.
To assess JADA’s comparative effectiveness over the balloon and standard of care, we relied on surrogate outcomes. We selected the need for massive transfusion (>4 units) as the primary endpoint and treated reduction in this risk as a proxy for the reduction in case fatality rates. The relative risk reduction for JADA versus the balloon is 86%, and 96% versus standard care7. Applying these probabilities to the projected number of PPH cases transitioning to JADA (either from balloon use or from the no-device group) yields an estimate of the number of PPH cases controlled with JADA and the number of fatalities averted.
To estimate deaths and DALYs averted, we applied a simplified assumption: women who would have died of PPH up to 2050 would all receive a device in the intervention scenario, with JADA increasingly replacing the balloon over time. These women therefore benefit from JADA’s associated reduction in mortality risk relative to the balloon (86%). For YLL, we used the average age of death from PPH in the US and multiplied it by life expectancy at that age, discounted to the year in which the death would have occurred. For YLD, we estimated that the probability of hysterectomy is ten times the probability of death and applied a total disability weight of 0.08 per case8. Total DALYs averted were then calculated as the sum of YLL and YLD, discounted at 2% per year to 2025 to reflect time preference. The temporary disability associated with hysterectomy was treated as occurring entirely in the year of the PPH case.
To estimate the health system cost impact, we relied on a recent study showing an average cost saving of $7,093 (2023 USD) per eligible patient when using JADA compared with the balloon9. After converting this estimate to 2025 USD and applying it to the projected number of PPH cases controlled under JADA, we obtain a total health-system saving of $4.5 billion.
To estimate productivity gains from averted deaths, we multiplied the remaining working years (retirement age minus age at death) by the probability of labour force participation and by US GDP per capita. The total additional cost of introducing JADA increases linearly with its growing share of PPH cases. While publicly available cost data for both devices are limited, available references suggest an approximate per-patient cost of $1,000 for JADA10 and $495 for the Bakri Balloon11.
Combining health-system savings, productivity gains, and the cost of scaling up the device yields a net health-system impact of –$5.3 billion. Dividing this by the total DALYs averted results in a negative ICER of $258,519, indicating that JADA is both cost-saving and health-improving.
Download a PDF of the case study11 https://www.preciousarrows.com/Bakri_Postpartum_Balloon_with_Rapid_Instillation_C_p/63028.htm