How ‘boom and bust’ Ebola R&D funding leaves us vulnerable
By Impact Global Health 29 May 2026
Introduction
As of 27 May 2026, the Bundibugyo virus outbreak in the Democratic Republic of Congo and Uganda has been declared a public health emergency of international concern by the WHO, with over 1,000 suspected cases and at least 238 suspected deaths reported across both countries. Yet behind these stark numbers lies a critical reality: the development of medical countermeasures (MCM) against orthoebolaviruses, of which the Bundinugyo strain is one, has progressed for others, but the Bundinugyo has been left behind.
Orthoebolaviruses include four major human pathogens: Zaire ebolavirus, Sudan ebolavirus, Bundibugyo ebolavirus, and Marburg virus, the latter being distinct from the ebolaviruses but also a deadly virus within the same family. Currently, there is an approved vaccine and antibody treatments for only the zaire ebolavirus. For other pathogens, there are no approved vaccines or therapeutics. However, for Sudan ebolavirus and Marburg virus, there are MCM candidates that have progressed to human testing, while Bundibugyo remains in early-stages of development.
Our analysis
We conducted a deep dive to better understand why there remains such a limited set of tools for the Bundibugyo strain. While there are existing filovirus products and candidates in development, these are heavily concentrated on other viruses and Ebola species, particularly Zaire Ebola, Sudan Ebola and Marburg virus. This leaves Bundibugyo with little to no dedicated product development activity, despite its outbreak potential.
New analysis from our product pipeline portal shows that, of the 94 filovirus candidates currently tracked, at least 50 target Zaire Ebola, 22 target Sudan Ebola, and 38 target Marburg virus. By contrast, none are specifically being developed for Bundibugyo Ebola.
This reflects a logical tendency in R&D to focus on the disease which has been the most prevalent – in this case, Zaire Ebola. But in doing so, it reveals how this can leave us unprepared for emerging strains.
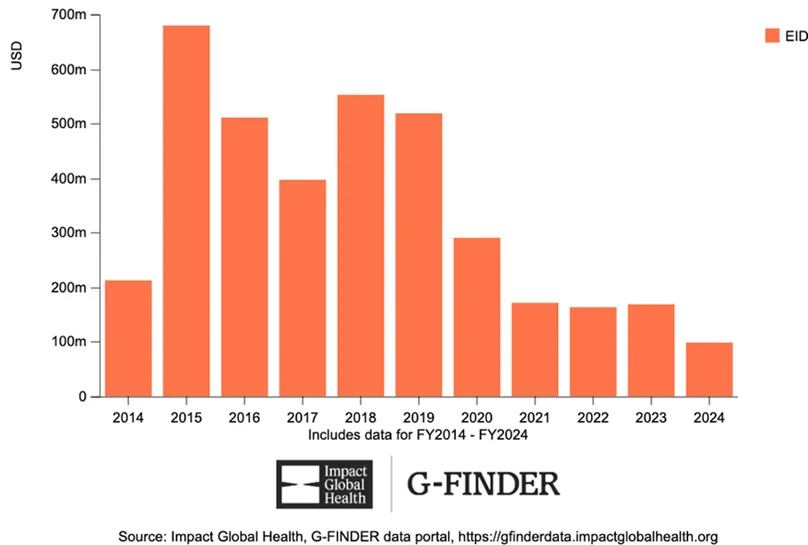
We also see this trend when we look at patterns of funding for Ebola R&D. Using our G-FINDER data, we see how funding spiked in 2015 following the Zaire Ebola outbreak in West Africa, jumping from US$213m to $679m before tailing off over the next decade to a low of $98m in 2024 (See Fig 1).
Figure 1: Global funding for Ebola R&D
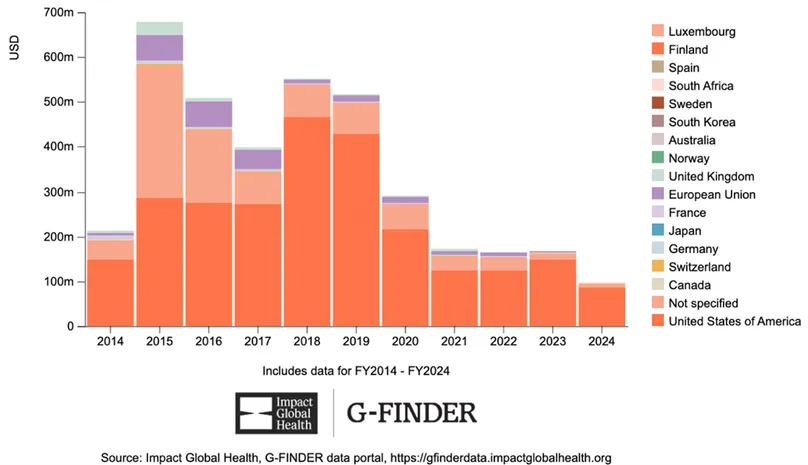
What’s more, R&D funding has become increasingly reliant on the US government. In 2015, it funded some 42% of Ebola R&D, rising to 88% in 2024. This overreliance creates a major fragility in the R&D ecosystem. A shift in US political priorities, budget allocations or global health engagement could quickly translate into a sharp contraction in Ebola R&D funding, leaving already neglected strains such as Bundibugyo even further behind (See Fig 2).
Figure 2: Funders of Ebola R&D
This ‘boom and bust’ approach to R&D funding is common across other emerging infectious diseases, and, whilst it is understandable given limited resources and the need to prioritise the greatest threats, it does leave gaps in the toolbox to tackle new outbreaks. In addition, any overreliance on a single source of funding creates obvious vulnerabilities for the ecosystem.
In partnership with the International Pandemic Preparedness Secretariat (IPPS), Impact Global Health has previously made the case for a more consistent and more balanced model of funding across a range of diseases with pandemic potential to better protect against future outbreaks.
All of that said, 'boom and bust' funding is still preferable to the 'perpetual bust' that many infectious diseases now face. Bundibugyo Ebola illustrates why. Because there are no dedicated Bundibugyo candidates in the current filovirus pipeline, scientists are now having to explore whether tools and platforms developed for other filoviruses can be adapted. One example is the Oxford Vaccine Group and Pandemic Sciences Institute’s work on outbreak-responsive vaccines for Sudan Ebolavirus and Marburg virus, which is now being drawn on in efforts relating to the Bundibugyo Ebolavirus outbreak in the DRC. Without the post-2014 surge in Ebola R&D investment, this kind of rapid adaptation pathway would likely be much thinner today.
We must look beyond short-term outbreak response and rebuild a system that is more balanced, better designed to anticipate threats, and able to draw on more consistent and diversified sources of funding. This means not only protecting core public and philanthropic investment, but also tapping into underused sources of finance, including diaspora networks, new health or solidarity taxes, regional financing mechanisms, and unconventional funders such as celebrity foundations and high net worth giving platforms. It also means reframing outbreak preparedness not only as a health issue, but as a security, economic resilience and development priority. Without this shift, the world will remain trapped between boom and bust for a small number of high-profile threats, and perpetual neglect for many others, leaving us even less prepared for the next outbreak.