From a multi-dose schedule to a single dose: how LMIC research can unlock the full potential of HPV vaccination
By Impact Global Health 18 June 2026
Context
Every breakthrough in global health sends ripples that reach far beyond borders. In an era of fiscal tightening and inward-facing policy priorities, investments in global health R&D are under increasing pressure. Yet these investments are among the most powerful drivers of innovation, economic growth, and resilience – not just for low- and middle-income countries (LMICs), but for high-income countries (HICs) as well. In the Ripple Effect project 1.0, Impact Global Health demonstrated that $71 billion in global health R&D funding from 2007-2023 catalysed $511 billion in GDP growth, 643,000 jobs, and 20,000 patents in HICs, a multiplier effect proving that global health investment drives domestic prosperity as well as global health outcomes. Building on this, the Ripple Effect 2.0 examined this dynamic through case studies of innovations initially developed for LMIC needs that later delivered measurable health and economic benefits in HICs. Now, the Ripple Effect 3.0 project extends this work by applying the same approach to five additional products, further strengthening the evidence base.
This case study focuses on the benefits of the human papillomavirus (HPV) vaccine moving from a two-dose schedule to a single dose for eligible individuals in the primary target group- girls aged 9-14 years. This change was based on innovative research from LMICs that is now being adopted in the UK and has huge potential for scale up across LMICs and HICs alike.
- A one dose HPV vaccine is just as effective as two. This evidence, generated in LMICs, is now reshaping immunisation policy and protecting more girls and young women in high-income countries.
- The simplified schedule has positive health impacts. By 2070, a one dose HPV vaccine schedule is projected to prevent an additional 2,700 cervical cancer cases, save almost 300 lives, and avert 12,700 DALYs in the UK, Europe, the US, and Japan.
- One-dose also generates significant economic returns – $1.5 billion in societal gains and $68 million in health system savings from averted cervical cancers across the UK, Europe, the US, and Japan by 2070.
- There are efficiency gains driven by reduced delivery costs from simplifying delivery to a single dose: moving from two doses to one translates to over $10 billion in delivery costs across these markets.
What is the HPV vaccine and why is it beneficial to move from a multi-dose vaccine schedule to a single dose schedule?
Human papillomavirus (HPV) causes virtually all cases of cervical cancer. It is the fourth most common cancer in women – causing the deaths of 350,000 women every year – most of whom, are in LMICs. The HPV vaccine has existed since 2006, moving from three doses to two by 2014 for eligible populations as part of a broader WHO drive to eliminate cervical cancer through 90% vaccination coverage in girls by age 15. Multiple schedules of two or three are still recommended for immunocompromised populations and those over 20 years by the WHO, although the age threshold does vary by country. A form of the vaccine (i.e. Gardasil, Cervarix and more) is now used in more than 128 countries.
For any vaccine schedule, including HPV, every additional dose creates barriers, such as higher costs, greater numbers of dropouts, and lower coverage generally - scenarios which disproportionately affect people in low-resource settings. A similarly efficacious, single-dose schedule effectively removes those barriers, making elimination a more realistic prospect rather than an ambition.
Innovation pathway
The question of whether a one dose HPV vaccine schedule could be enough emerged from an accidental observation: in the Costa Rica HPV Vaccine Trial, women who had received only one dose appeared just as protected as those who had received three, with antibody levels stable for over a decade. Similar findings followed from trials in India. Building on this observation, dedicated trials across Kenya, Tanzania, and a further trial in Costa Rica confirmed that a single dose offered equivalent protection against the HPV strains responsible for around 90% of all cervical cancers. In 2022, the WHO endorsed a one-dose schedule for eligible individuals, with HICs such as the UK and Australia implementing this from 2023 and the US revising its schedule recommendation in 2026.
Fewer doses mean more people protected. Evidence from general childhood immunisation programmes shows that reducing the number of required contacts is associated with higher completion rates. The same logic applies here. A study in the US found that while 79.1% of adolescent girls had received at least one HPV vaccine dose, only 64.3% had completed the full series; a gap of nearly 15 percentage points. That drop-off is not random: people in more socioeconomically disadvantaged areas are significantly less likely to complete a multi-dose schedule, meaning the impact falls hardest on those with the least. Moving to one dose simplifies delivery, reduces cost, and removes drop-out. In the UK, moving to one dose in 2023 was followed by a 1.6 percentage point increase in uptake among 12-year-old girls compared to the previous year. For HICs and LMICs alike that have not yet reached elimination targets, a one-dose HPV vaccine schedule offers a practical route to closing the coverage gap and bringing the elimination of cervical cancer within reach. It also offers significant societal and economic returns.
Health impact in the EU, UK, US and Japan
Across the EU, UK, US and Japan – key HIC markets selected in this study for their substantial impact and strong data availability – we estimate that, through a one dose vaccination program to 2050, an additional 2,600 cervical cancer cases could be averted, saving almost 300 lives and averting 12,700 DALYs by 2070 compared to a two-dose schedule.
Because the health benefits of vaccination materialise decades after receiving the vaccine, we extended our time horizon to 2070 to capture the full impact, while limiting vaccination itself to the period up to 2050. This long delay also means that discounting has a substantial effect, reducing the DALYs averted by approximately threefold when discounted back to 20251.
The health impact is driven by the incremental effective coverage of one-dose compared to two-doses of the HPV nonavalent vaccine targeting 9 HPV strains, of which 7 are cancer causing HPV strains (16/18/31/33/45/52/58), where a marginal but non-significant difference in vaccine effectiveness is offset by an increased uptake in the female population due to the reduced schedule. We have modelled this increased uptake and therefore completion of a single dose schedule on a conservative 1.6 percentage point increase relative to the two-dose coverage based on data from the UK. More optimistic uptake scenarios, assuming 3 or 5 percentage point increases in coverage, project up to 7,500 and 14,300 additional cervical cancer cases averted by 2070, highlighting the significant potential of a one-dose schedule to reduce the cervical cancer burden.
Table 1: Potential health impact from switching to one dose in the EU, UK, US, and Japan
Figure 1: Additional cervical cancer cases averted following the switch to a single dose schedule
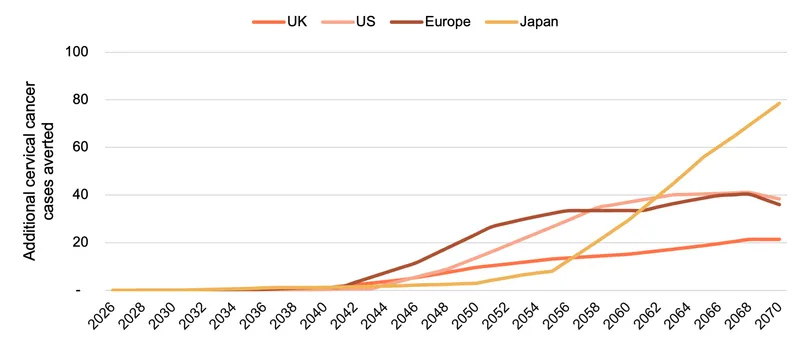
Switching from a two-dose to one-dose generates meaningful incremental health gains across all four regions. While the effects modelled for the UK demonstrate projected impact based on the real-world ‘switch’ from a two to one dose schedule in 2023, Europe and Japan have yet to make this transition. and in the US, the real-world impact of updated guidelines is in its infancy. The health impacts for these latter three demonstrate a stylised scenario where collectively almost 2,300 additional cervical cancer cases could be averted. Europe records the largest potential gains in cervical cancer cases averted, driven by population size and high baseline burden across the region. Japan, despite having the smallest vaccinated population of the four regions, shows the greatest potential impact on averted mortality and DALYs, reflecting its greater underlying cervical cancer mortality rates and substantially higher baseline HPV prevalence, a consequence of the 2013–2022 programme suspension which left a large cohort of women unvaccinated and cycling through peak infection and cancer risk years.
Economic Impact in the EU and UK
Being alive and in good health has a value to the individual and to society. Using the Value of a Statistical Life approach, we estimated the societal gains to be worth close to US $1.5 billion[1] across our four markets.
The benefits of switching to one dose extend well beyond the lives saved – the change also delivers significant cost savings. The modest increase in cancers averted – driven by slightly higher coverage – translates into over $68 million in savings across our four markets: $38 million in the US, $15 million in Europe, above $10 million in Japan and nearly $6 million in the UK. These figures are expressed in 2025 USD, adjusted downward to reflect the fact that a dollar saved in the future is worth less than a dollar saved today. Without that adjustment, the savings are roughly twice as large.
Table 2: Potential health system cost savings (USD 2025) from switching to one dose in the EU, UK, US, and Japan
Cost savings do not stop there. The primary driver of savings is in the cost of the vaccine itself: administering one dose instead of two cuts procurement costs roughly in half. Further savings from fewer clinic visits, reduced cold-chain logistics, and lower staffing requirements contribute, but the vaccine cost accounts for the majority. The result: programme delivery costs are nearly halved. More precisely, the gains in delivery costs are estimated at over $10 billion across the four markets: $6.3 billion in the US, $3.1 billion in Europe, $547 million in Japan and $369 million in the UK. For health systems already under pressure, these are precious resources that can be redirected to other priority areas.
Figure 2: Total health system savings over time from cervical cancers averted and reduced vaccine rollout costs following the switch to a single dose schedule
-808x439.webp)
[1] For ease of comparison, all monetary values are reported in inflation-adjusted 2025 US dollars
Conclusions
The evolution of the HPV vaccine from a multi-dose to a single dose schedule – driven by research in and for LMIC markets – demonstrates how global health R&D can stimulate high-impact opportunities beyond their original context. Research conducted in LMICs did not just solve a problem in low-resource settings, it unlocked a simpler and more equitable path to cervical cancer elimination through the potential to increase coverage while decreasing costs and easing pressure on health systems in all contexts. A disease that kills 350,000 women a year is now likely within realistic reach of being eliminated, and that prospect owes as much to LMIC-driven research as it does to the vaccine itself.
Key assumptions
The projected health impact of switching from a two-dose to a one-dose HPV vaccination programme follows clear programmatic and epidemiological logic. The model tracks each female birth cohort vaccinated at age 12 from the respective region's one-dose switch year through to 2050, with health outcomes projected to 2070. This extended horizon is necessary because cervical cancer typically develops 10 to 15 years after HPV infection; most of the health benefit from vaccines given today will not materialise until the 2035 to 2055 window when vaccinated cohorts reach peak cervical cancer risk ages of 35 to 55.
The epidemiological foundation of the model is cervical cancer incidence and mortality data sourced from the Global Burden of Disease (GBD), adjusted using national registry scalers to align with country-reported rates where GBD estimates diverge from domestic surveillance data. These scaler-adjusted counts form the basis from which all downstream health outcomes (cases averted, deaths averted, and DALYs) are derived. Of all cervical cancer cases, 90% are attributable to the seven cancer causing HPV strains targeted by the nonavalent vaccine (16/18/31/33/45/52/58), a figure derived by combining the established finding that 99.7% of cervical cancers are caused by HPV with the type-specific attribution of approximately 90% for nonavalent strains. This fraction is applied uniformly across all regions and age bands to translate the GBD cervical cancer burden into the HPV-attributable cases and deaths that the HPV vaccination can prevent. Post-2023 burden is projected forward using a linear trend extrapolated from the adjusted historical GBD data, subject to a regional floor of 10% of the 2023 baseline to prevent implausibly optimistic projections as vaccination programmes mature. While the HPV vaccine is commonly given to girls and boys, we have modelled the female-only impact due to the focus on cervical cancer as the primary outcome, as well as only considering those in the target cohort for the vaccine (i.e. not catch-up groups age 15+ years). We have not included other forms of cancer in our modelling, nor have we modelled for herd immunity or transmission dynamics, meaning the results presented here are likely a considerable underestimate.
The comparisons modelled differ by region, reflecting each country's actual policy history. For the UK and US, the counterfactual is grounded in real policy decisions: the UK switched to a one-dose schedule in 2023/24, and the US updated guidelines in 2026, and the model compares each country's actual one-dose programme against a continuation of the two-dose schedule from that switch year. For Europe and Japan, no such switch has yet occurred, and the comparisons are forward-looking stylised scenarios. For Europe, we model the incremental impact of a hypothetical switch to one dose in 2023/24, in line with the UK, against the two-dose programmes currently in place. It is important to note that European HPV vaccination coverage is highly heterogeneous, we have applied a last-dose coverage of 62.8% for the two-dose counterfactual which is weighted by 10–19-year-old female population across EU/EEA countries. For Japan, we model the impact of adopting a one-dose schedule at the 2023 reintroduction of the national HPV programme, following a nine-year suspension from 2013 to 2022, compared to a counterfactual, real-world experience where that reintroduced programme proceeded on a two-dose basis for the primary target population.
The case for switching to one dose rests on a straightforward trade-off of efficacy vs uptake. Vaccine efficacy is sourced from Kreimer et al. (2025): 94.5% for one dose and 95.8% for two doses against the seven HPV strains responsible for approximately 90% of cervical cancer cases; a difference that is not statistically significant. Both schedules are modelled as providing lifelong protection, consistent with 16-year immunogenicity data. The health benefit of switching therefore comes primarily from uptake: a simpler single-appointment schedule increases programme completion by 1.6 percentage points, derived from UK UKHSA data comparing two-dose and one-dose years. This is potentially conservative; US data shows a gap of nearly 15 percentage points between first-dose uptake and schedule completion. Because the small VE penalty applies only to those already being vaccinated, while the uptake gain reaches those who previously dropped out, the net effect is positive across all regions.
To quantify the economic benefits of switching from a two-dose to a one-dose HPV vaccination schedule, we estimated three categories of savings: health system cost savings from averted cervical cancers, programme delivery cost savings, and the broader societal value of healthy life-years gained.
Health system cost savings. We gathered estimates of the lifetime cost of treating a cervical cancer case from published literature for each of the four markets. These costs were originally reported in different currencies and reference years – GBP 2023 for the UK (£22,184), USD 2018 for the US ($82,100), EUR 2011 for Europe (€24,276), and USD 2022 for Japan ($26,700). [1] To enable comparison, we converted all values to a common currency (USD) using exchange rates and adjusted for inflation to express them in 2025 dollars. We then multiplied the cost per case by the number of additional cancers averted each year under the one-dose scenario, from 2026 through 2070. All future savings were discounted back to 2025 using an annual discount rate of 2%.
Programme delivery cost savings. The cost of delivering the vaccine comprises the price per dose and an administration fee. By moving from two doses to one, both components are reduced for each individual vaccinated. We sourced market-specific vaccine prices – £57.80 per dose in the UK, $337 in the US, $82 in Europe, and $166 in Japan – and converted them to 2025 USD. Recognising that vaccine prices are unlikely to remain static, we modelled a price decline over time to reflect the entry of competitors: a 15% reduction in the year following patent expiry, followed by a gradual annual decline until the price reaches a floor equivalent to 55% of the current market-specific cost. This correction factor was applied year by year from 2023 to 2050 and combined with projected cohort sizes to estimate annual delivery cost savings. As with the health system savings, all values were discounted to 2025 at a 2% annual rate.
Societal value of health gains. To capture the broader value of improved health beyond direct cost savings, we applied a Value of a Statistical Life Year (VSLY) approach. The VSLY reflects how much society is willing to pay for marginal reductions in mortality risk, derived primarily from wage-risk trade-offs in labour markets. We applied region-specific VSLY estimates to the discounted DALYs averted in each market. This yielded an aggregate societal value of approximately $1.5 billion across the four markets.
Time horizon and discounting. Our model captures vaccination costs through 2050 but extends the health benefit horizon to 2070, reflecting the long latency between HPV vaccination and the cervical cancers it prevents. All monetary values are reported in inflation-adjusted 2025 US dollars, and future costs and benefits are discounted at 2% per year back to 2025.
For full data, visuals and methodology, visit: impactglobalhealth.org/ripple-effect
[1] The estimate for Japan is based on point-of-diagnostic costs and is therefore likely to be an underestimate. The estimate for Europe is based on a study conducted in Italy.